

It’s been said a million times: Appalachia is often presented as a monolith. From presenting it as uniformly white, rural, and poor to conceiving of the coalfields as the “real Appalachia,” writers have often made a vast, diverse area seem like it’s all the same. In fact, Appalachia stretches from the southern New York foothills to the Atlanta suburbs and is home to 25 million people living in 13 different states in all kinds of situations.
Nothing underlines Appalachia’s regional diversity—and inequality—quite as starkly as COVID-19. Although the coronavirus is neutral as to who it infects, factors like geography, race, class, and political leadership have all shaped how the virus has spread throughout the region. While some areas have so far avoided the brunt of COVID-19’s impact, others are experiencing dramatic outbreaks requiring intervention.
As of April 18, Appalachia had 20,671 reported COVID-19 cases (about 83 infections per 100,000 people) and 765 deaths, about 3.7 percent of all people infected. As a whole, Appalachia’s outbreak is relatively small compared to the entire U.S., which reported 234 infections per 100,000 people and a 4.6 percent death rate the same day. However, if one digs down to the state and county level, it’s clear that some Appalachian communities have already been ravaged by the disease, and the situation may only be getting worse.

Figure 1: COVID-19 Cases in Appalachian Regional Commission counties by state (as of April 18). Via expatalachians and Johns Hopkins University.
Looking at the raw number of coronavirus cases in Appalachia by state (Figure 1), Appalachian Pennsylvania accounts for over a third of the region’s caseload with about 7,000 cases. It is followed by the southern regions of Georgia and Alabama, each with over 2,500 cases, and Ohio and Tennessee with over 1,000 cases each. State cases then begin to level and taper off, with most remaining states having between 500 and 1,000 cases. Appalachian Maryland has the lowest number of infections, with just 153 cases.
Overall, this picture makes sense. Pennsylvania, Alabama, Georgia, Tennessee, and Ohio are also the five most populous areas of Appalachia, and each is home to at least one major urban center like Pittsburgh, Birmingham, or Knoxville that has served as an epicenter for the outbreak. However, COVID-19 isn’t simply the product of population or density. While useful in providing an orientation on the regional outbreak, raw numbers can hide as much as they reveal.
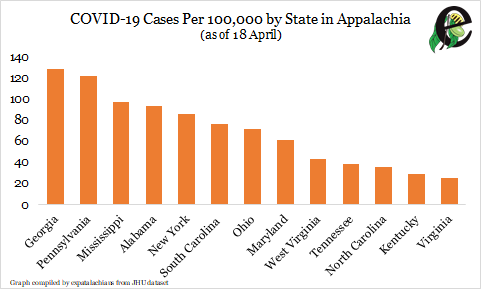
Figure 2: COVID-19 Cases Per 100,000 People by State in Appalachia (as of April 18). Via expatalachians and Johns Hopkins University.
Controlling for population illuminates the situation a bit. Figure 2 shows the number of COVID-19 cases in each Appalachian area for every 100,000 people, a common way in public health to compare infection rates. It’s then easier to compare a place like Appalachian Pennsylvania (pop. 6 million) with Appalachian Maryland (pop. 250,000).
And the results are revealing. When adjusted for population, Appalachian Pennsylvania, which in absolute numbers has almost twice as many cases as the next state, actually falls into second behind Appalachian Georgia’s 129 cases per 100,000 people. Other populous states, like Ohio and Tennessee, also have much lower infection rates. Looked at in this way, the biggest regional outbreaks are actually in Pennsylvania, New York, and Deep South states like Georgia, Mississippi, Alabama, and South Carolina. This begs the question: Why these states?
Part of the answer concerns geography and regional economies. By virtue of their position in the world economy, transportation hubs like New York City and Atlanta were seeded with coronavirus early on, contributing to their development into hotspots. Proximity to these hotspots may help explain why Appalachian Pennsylvania and Georgia have high infection rates, with two populous Pennsylvania counties near New York City registering over 500 cases per 100,000 people.
Conversely, Central Appalachian counties’ smaller prominence in world travel may have delayed the arrival of the virus. However, rural Appalachians shouldn’t think they’re out of the woods yet. Much like the region’s experience with the 1918 Spanish flu, some fear it is only a matter of time before more rural areas with less developed health infrastructures are hit hard by the virus. Indeed, this trend may already be emerging, with six of the top 10 most-infected Appalachian counties having fewer than 100,000 people.
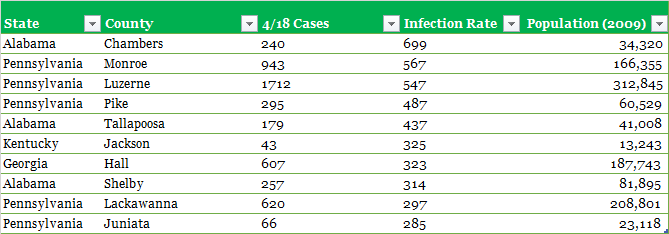
Figure 3: Table of ten counties with the highest COVID-19 infection rate per 100,000 people as of April 18. Via expatalachians and Johns Hopkins University.
Race and class are also major factors in explaining the virus’ spread. Preliminary data indicates that black Americans are being affected at rates far exceeding their white compatriots, with factors like greater economic insecurity, lack of access to healthcare, and chronic illnesses associated with structural racism contributing to both higher infection and death rates among African Americans. Despite comprising only 13 percent of the U.S. population, black people accounted for 30 percent of all U.S. COVID-19 patients with reported race on April 17, with black people dying at rates two or three times their white counterparts in some cities.
COVID-19’s disproportionate impact on black communities may help explain why some southern Appalachian states like Alabama, where African Americans make up 25 percent of the population (compared to 4 percent in W.V.), have been especially hard hit. In particular, Birmingham, one of the largest cities in Appalachia and where African Americans make up 70 percent of the population, has been singled out as an example where longstanding neglect of black Americans could result in New York City-level infection rates. While coverage of COVID-19 in Appalachia has often focused on predominantly white rural areas, any effective solution will necessarily incorporate the virus’ disproportionate impact on the region’s people of color.
Finally, one of the most important factors in determining COVID-19’s spread throughout Appalachia has been the different choices made by state and local leaders in combating the virus. With the federal government largely abdicating leadership for much of the COVID-19 crisis, state governors in particular have been tasked with deciding when and to what extent they implement social distancing measures, which have been proven to prevent COVID-19’s spread. While some Appalachian states like Ohio and Kentucky have been hailed as national trendsetters for implementing social distancing early, others states Georgia and South Carolina have been criticized for implementing weaker measures much later.
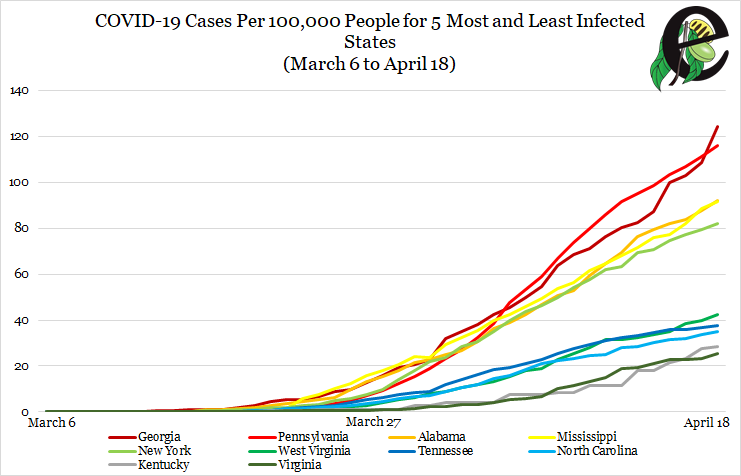
Figure 4: COVID-19 Cases per 100,000 People for the Five Most and Five Least COVID-19 Infected States. States that instituted statewide stay-at-home orders on or after April 1 (Georgia, Pennsylvania, Alabama, Mississippi) are in shades of red or orange. States that instituted stay-at-home orders before April 1 are in shades of green, blue, or gray. With the exception of Appalachian New York, there is a noticeable divergence between the two groups’ trajectories. Via expatalachians and Johns Hopkins University.
As Figure 4 illustrates, these choices may have drastically altered the course of the outbreak in different states. With the exception of New York, the epicenter of the US COVID-19 outbreak, all of the top five most affected states in Appalachia issued stay-at-home orders in April, relatively late, while all of five least affected states implemented them in March, sometimes a week or two earlier than their later counterparts. Although the exact effect of social distancing versus other factors has yet to be determined, these preliminary trends suggest state action can mitigate COVID-19’s impact across Appalachia.
However, whether the costs of social distancing are worth the mitigation remains a point of contention within the region. Despite a vast majority of Americans supporting continued social distancing and a recent Harvard study stating the US needs far more testing to safely lift restrictions, some southern Appalachian states are already planning a limited reopening for businesses on or before May 1.
Whatever comes of these and future developments, the multifaceted situation surrounding COVID-19 in Appalachia merits a more nuanced discussion of regional challenges and solutions.
For weekly updates on the COVID-19 outbreak in Appalachia, bookmark our COVID-19 in Appalachia Tracker, updated every Thursday.
Nicholas Brumfield is a native of Parkersburg, WV currently working in Arlington, VA. He also comes from a proud family of nurses, including his sister and aunt. For more hot takes on Appalachia and Ohio politics, follow him on Twitter: @NickJBrumfield.
Subscribe to The Patch, our newsletter, to stay up-to-date with new expatalachians articles and news from around Appalachia.
